Printable Workplace Accident Report Form
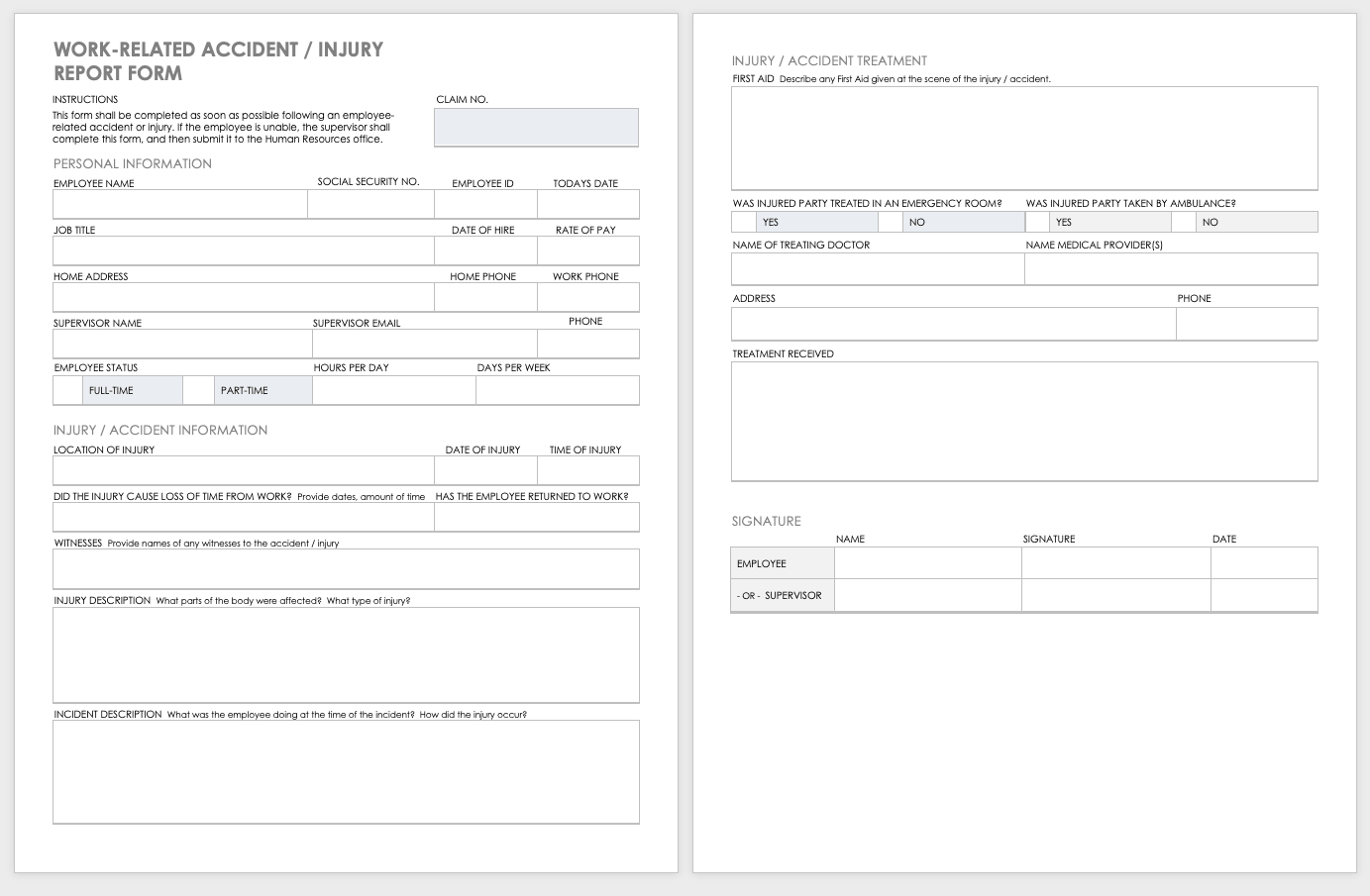
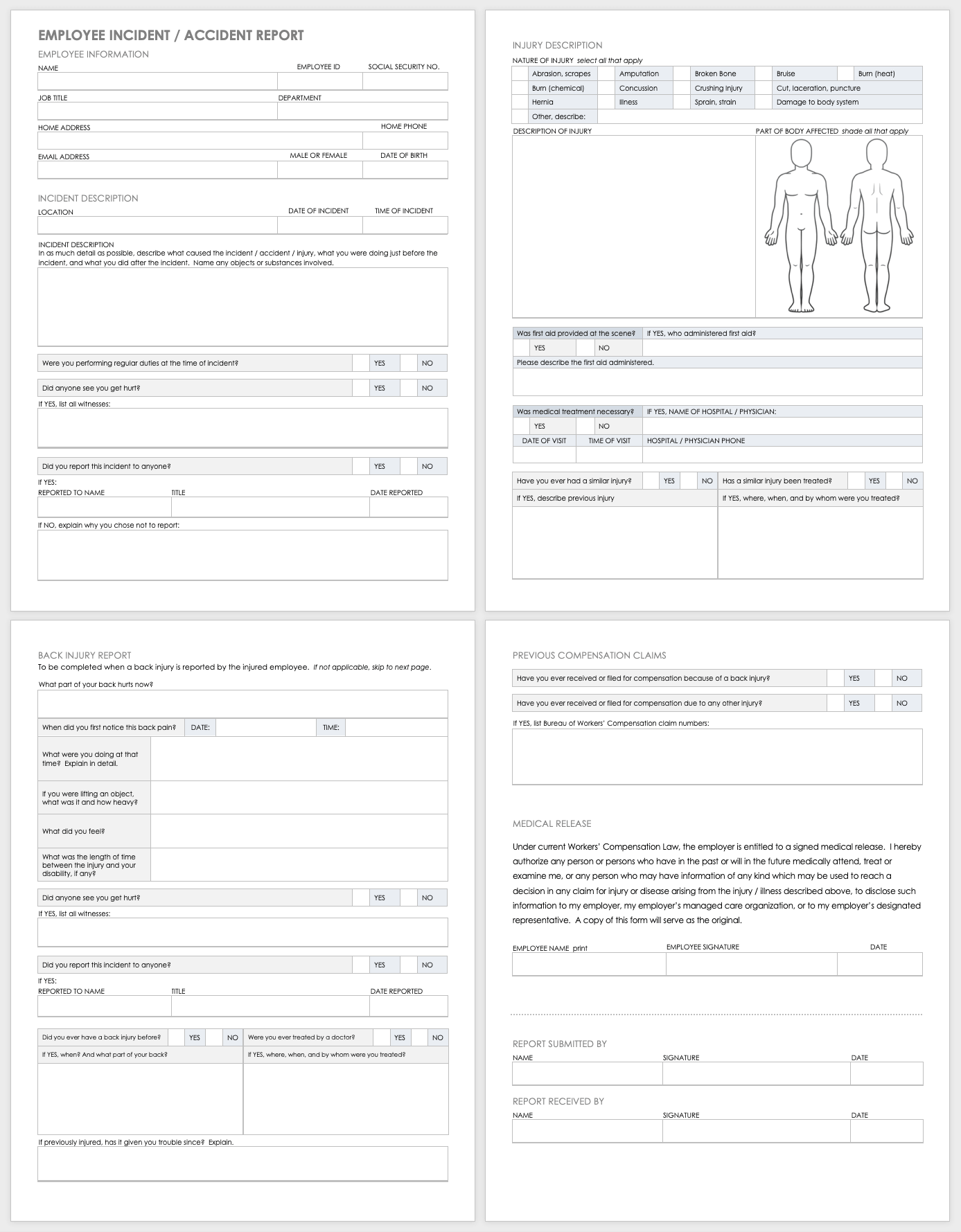
Printable Workplace Accident Report Form - If the employee is unable, the supervisor shall complete this form, and then submit it to the human resources office. It shall be completed in a timely manner following an incident, and can also be used to investigate a near miss This form is to be completed by the supervisor of an employee that has experienced an incident resulting in a serious injury or illness. In as much detail as possible, describe what caused the incident / accident / injury, what you were doing just before the incident, and what you did after the incident. In order to complete a timely and thorough Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. Name any objects or substances involved. Statement of witness to accident incident identification information name of employee alleging incident title / role shift department witness statement your name was provided as a witness by the employee listed above. Return completed form to : Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. Statement of witness to accident incident identification information name of employee alleging incident title / role shift department witness statement your name was provided as a witness by the employee listed above. If the employee is unable, the supervisor shall complete this form, and then submit it to the human resources office. This form is to be completed by the supervisor of an employee that has experienced an incident resulting in a serious injury or illness. Personal information employee name social security no. Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. Included on this page, you will find an employee incident/accident report form, a supervisor's incident investigation report template, a statement of witness to accident template, an employee's return to work plan, and many more helpful workplace accident report forms. Name any objects or substances involved. It shall be completed in a timely manner following an incident, and can also be used to investigate a near miss This form serves to document select all that apply Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. In as much detail as possible, describe what caused the incident / accident / injury, what you were doing just before the incident, and what you did after the incident. Fill out this form to report a workplace incident that resulted in. In as much detail as possible, describe what caused the incident / accident / injury, what you were doing just before the incident, and what you did after the incident. Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. In order to complete a timely and thorough Fill out this form. If the employee is unable, the supervisor shall complete this form, and then submit it to the human resources office. In as much detail as possible, describe what caused the incident / accident / injury, what you were doing just before the incident, and what you did after the incident. Name any objects or substances involved. Fill out this form. Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. If the employee is unable, the supervisor shall complete this form, and then submit it to the human resources office. Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. In order to complete. It shall be completed in a timely manner following an incident, and can also be used to investigate a near miss Statement of witness to accident incident identification information name of employee alleging incident title / role shift department witness statement your name was provided as a witness by the employee listed above. In as much detail as possible, describe. In order to complete a timely and thorough Name any objects or substances involved. Personal information employee name social security no. Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. Statement of witness to accident incident identification information name of employee alleging incident title / role shift department witness statement your. Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. In as much detail as possible, describe what caused the incident / accident / injury, what you were doing just before the incident, and what you did after the incident. In order to complete a timely and thorough It shall be completed. In order to complete a timely and thorough This form is to be completed by the supervisor of an employee that has experienced an incident resulting in a serious injury or illness. Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. It shall be completed in a timely manner following an. Personal information employee name social security no. Included on this page, you will find an employee incident/accident report form, a supervisor's incident investigation report template, a statement of witness to accident template, an employee's return to work plan, and many more helpful workplace accident report forms. This form is to be completed by the supervisor of an employee that has. Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. Included on this page, you will find an employee incident/accident report form, a supervisor's incident investigation report template, a statement of witness to accident template, an employee's return to work plan, and many more helpful workplace accident report forms. This form is. In as much detail as possible, describe what caused the incident / accident / injury, what you were doing just before the incident, and what you did after the incident. If the employee is unable, the supervisor shall complete this form, and then submit it to the human resources office. Return completed form to : Fill out this form to report a workplace incident that resulted in injury, illness, or a near miss. In order to complete a timely and thorough It shall be completed in a timely manner following an incident, and can also be used to investigate a near miss Included on this page, you will find an employee incident/accident report form, a supervisor's incident investigation report template, a statement of witness to accident template, an employee's return to work plan, and many more helpful workplace accident report forms. Personal information employee name social security no. Name any objects or substances involved. This form is to be completed by the supervisor of an employee that has experienced an incident resulting in a serious injury or illness.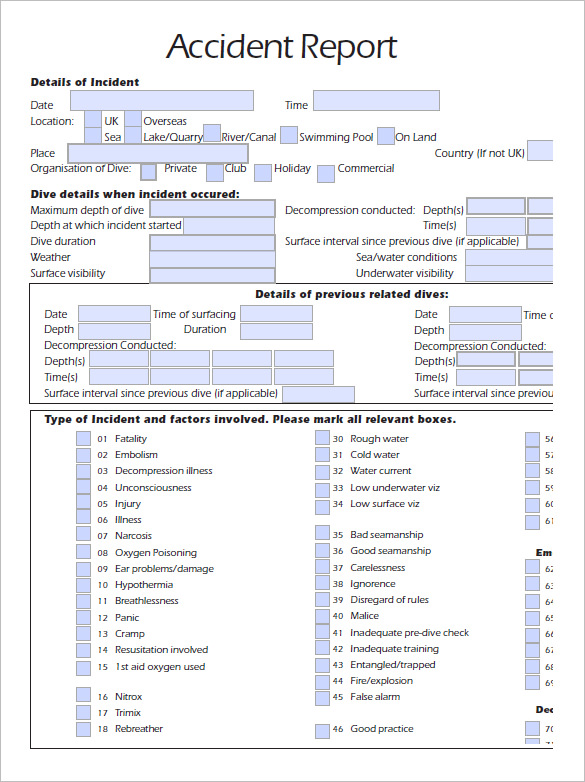
Accident Report Template 10+ Free Word, PDF documents Download Free
Employee Accident Report Form (Free PDF Template)
Free Incident Report Template PDF & Word Legal Templates
Employee Accident Report Form Printable Printable Forms Free Online
Free Workplace Accident Report Templates Smartsheet
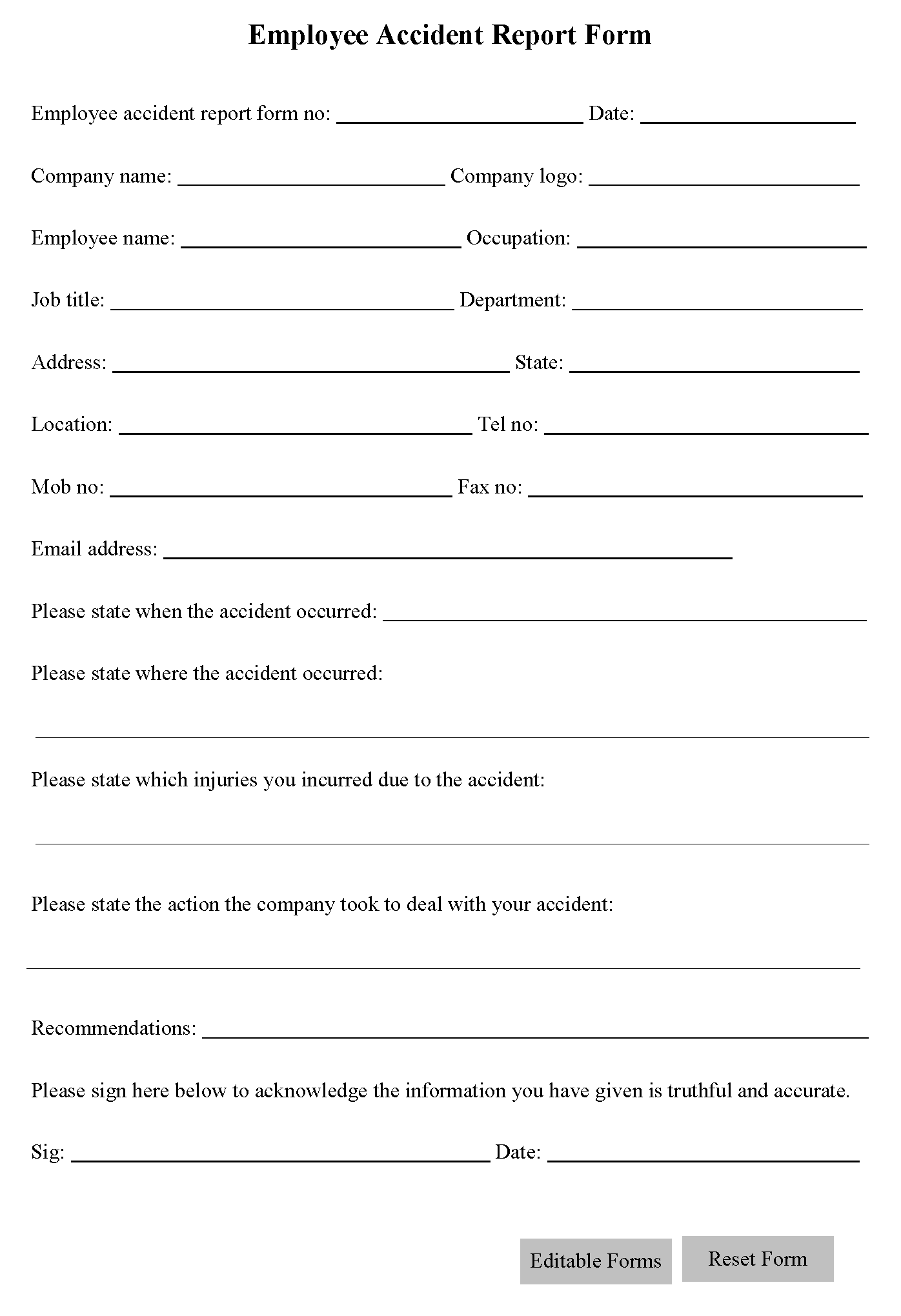
Employee Accident Report Form Editable Forms
Free Workplace Accident Report Templates Smartsheet

Printable Accident / Incident Report Forms Template for Work Etsy
Free Workplace Accident Report Templates Smartsheet
Free Workplace Accident Report Templates Smartsheet
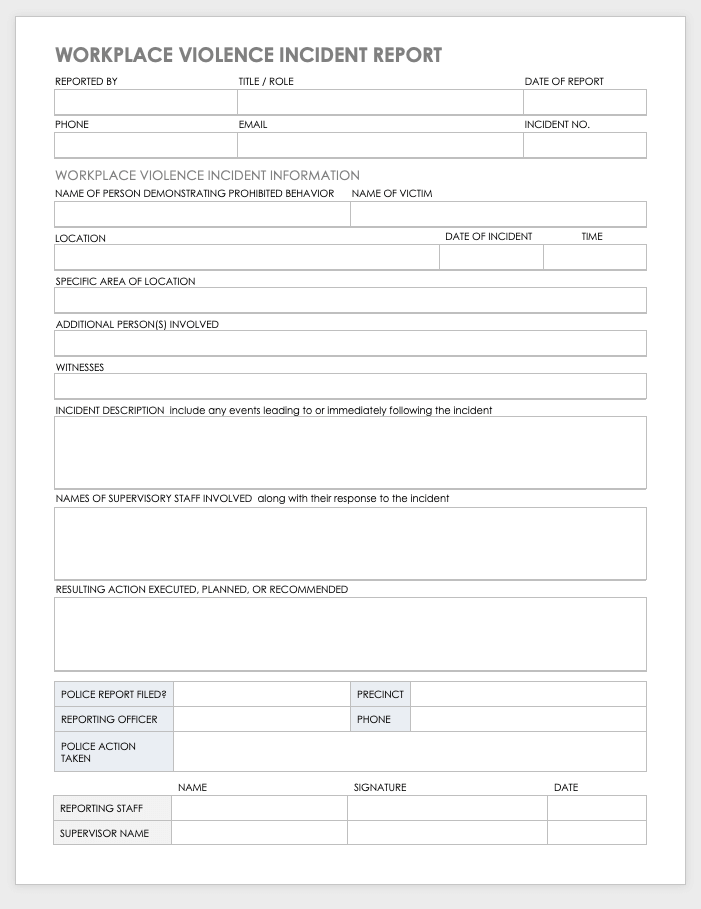
Statement Of Witness To Accident Incident Identification Information Name Of Employee Alleging Incident Title / Role Shift Department Witness Statement Your Name Was Provided As A Witness By The Employee Listed Above.
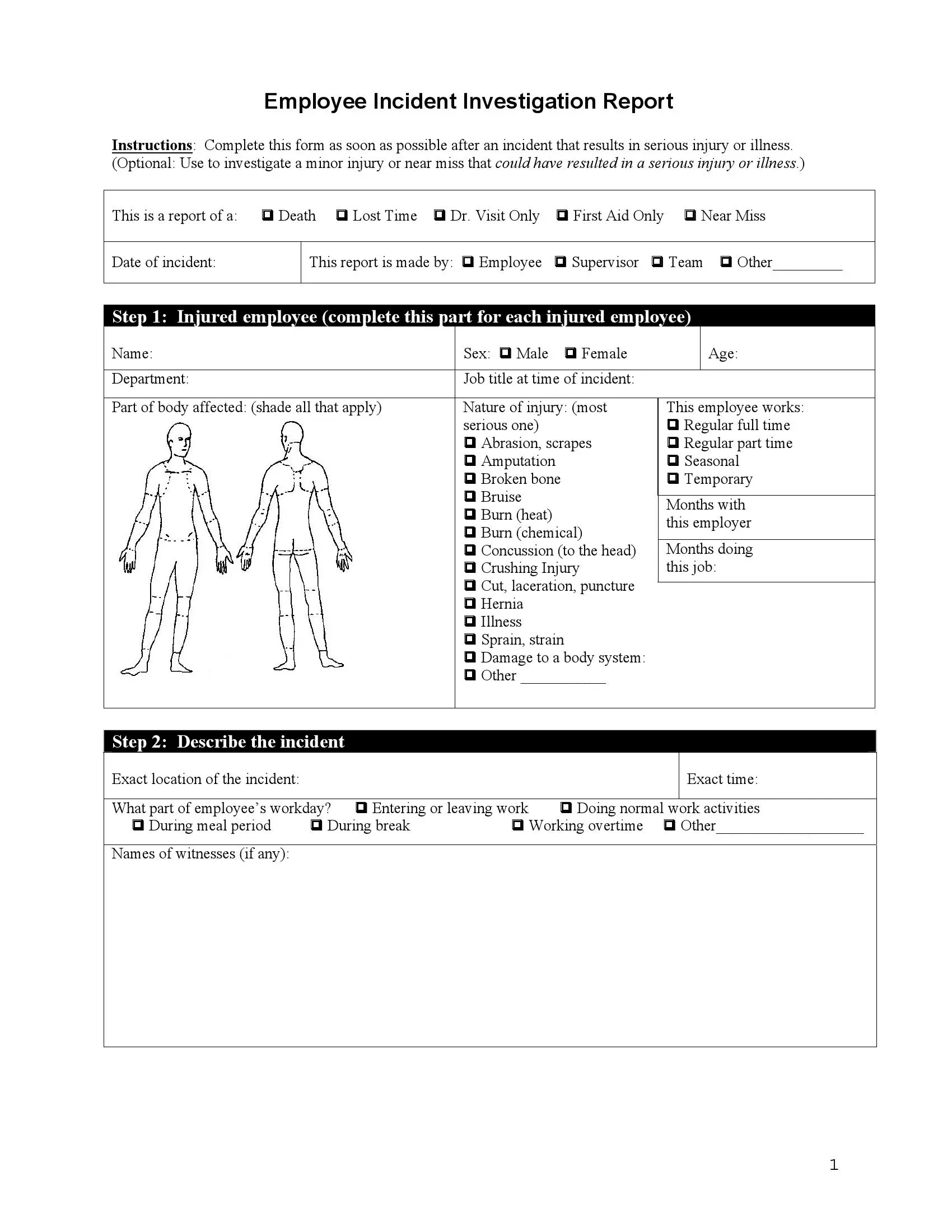
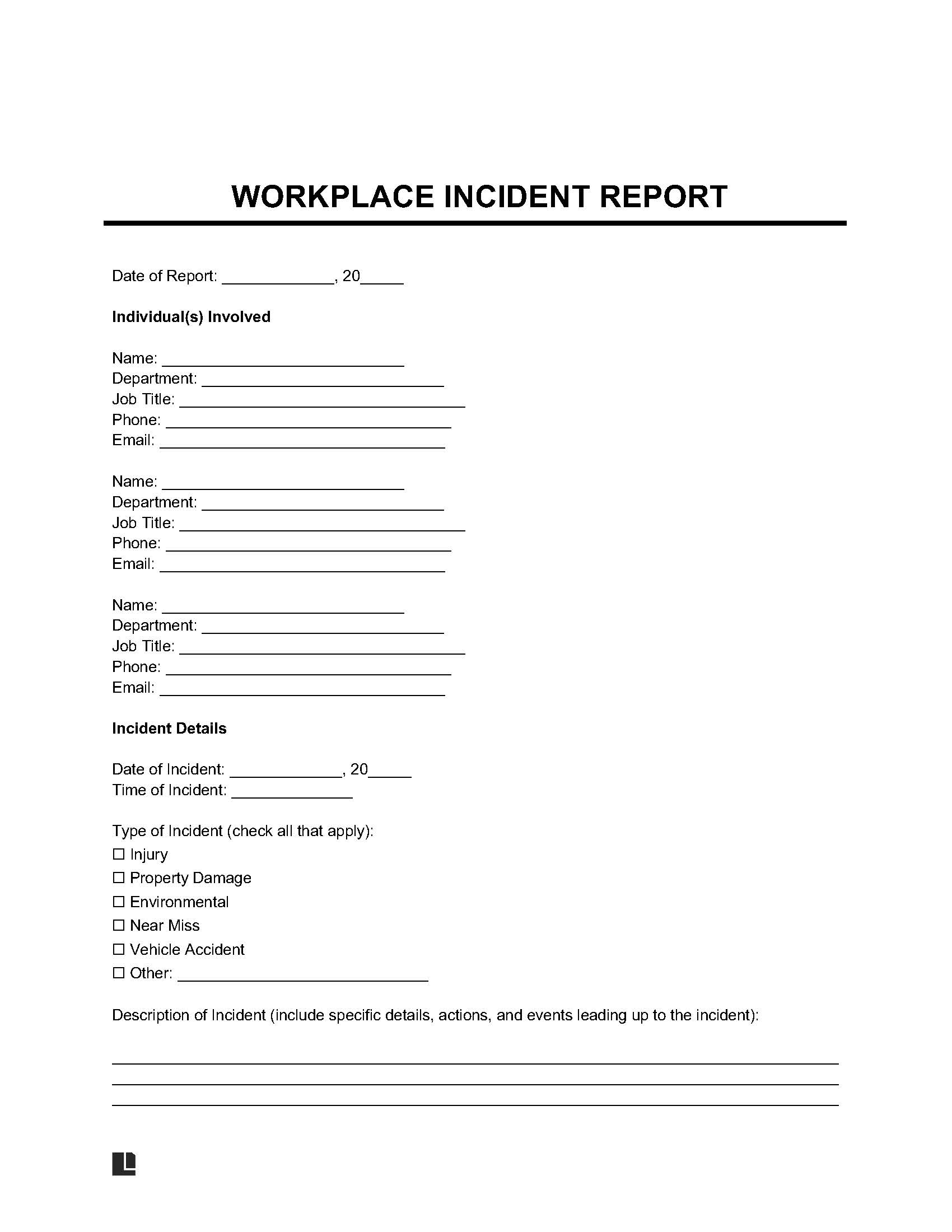
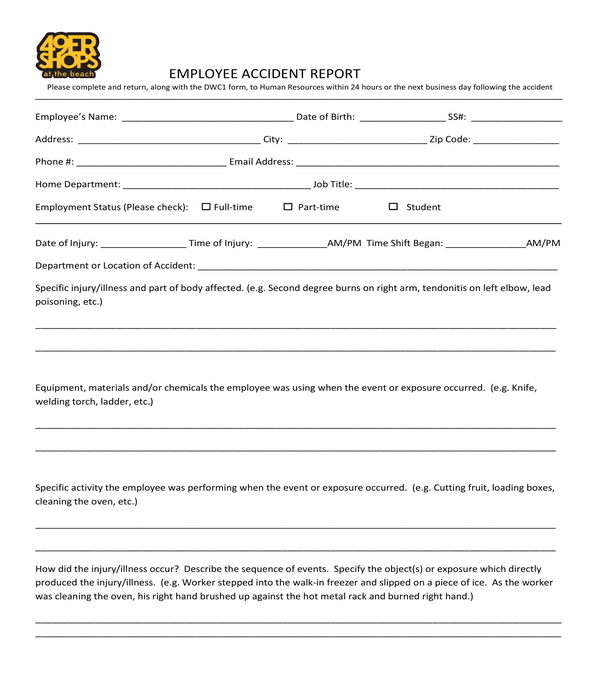
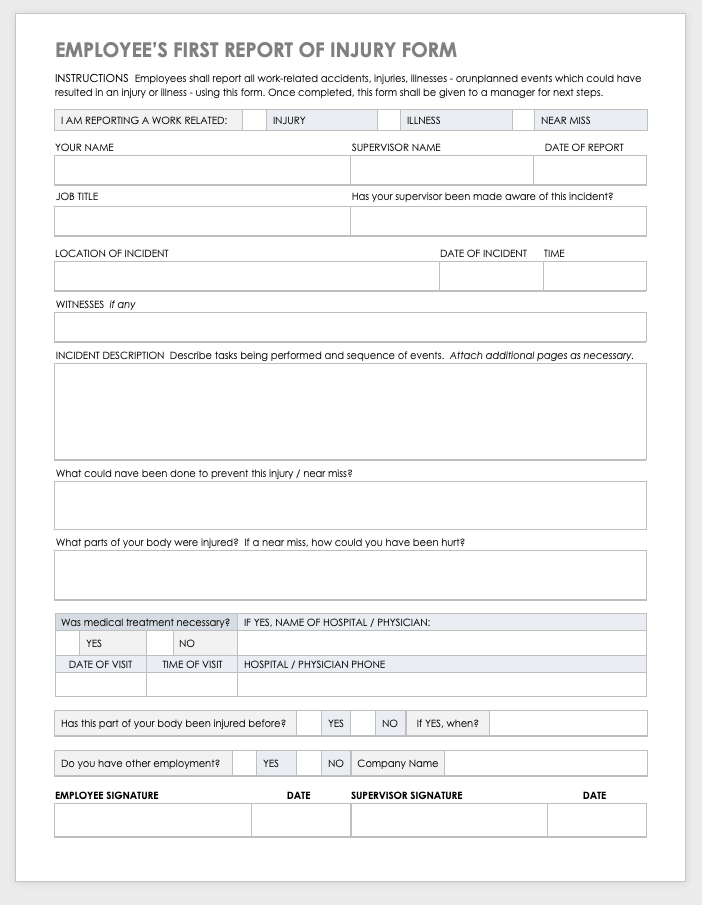
Fill Out This Form To Report A Workplace Incident That Resulted In Injury, Illness, Or A Near Miss.
This Form Serves To Document Select All That Apply
Related Post: